I’ll be giving the keynote at the FSU College of Medicine’s Business & Medicine Symposium in Tallahassee this Saturday. If you’re a student there, make sure to come say hi during the morning coffee or lunch after!
From MONETIZING MEDICINE: PRIVATE EQUITY AND COMPETITION IN PHYSICIAN PRACTICE MARKETS, a report by the American Antitrust Institute:
Price increases associated with PE acquisitions are exceptionally high where a PE firm controls a competitively significant share of the local market. When we focus our analysis on markets where a single PE firm controls more than 30% of the market, we find further elevated prices associated with PE acquisitions in each of the 3 specialties with statistically significant results, for gastroenterology (18%), obstetrics and gynecology (16%), and dermatology (13%).
Discussed in the NYTimes here.
This chart comes from a Joint Commission paper on Physician Task Load and the Risk of Burnout:
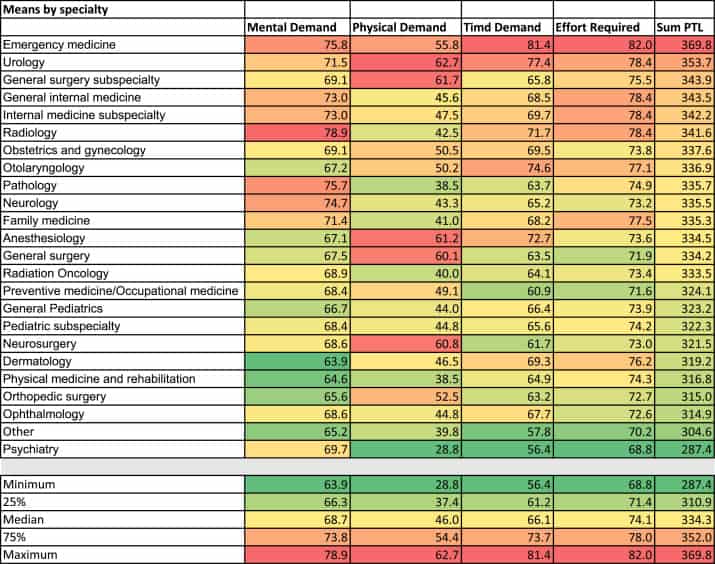
It reads like a meaningful comparison, but the data is actually just self-reported from a survey of different specialties. It is a (nonetheless flawed) reflection of how these groups of doctors viewed themselves, their work, and its challenges.
The paper came out in 2021 but this feels dated. I think Time Demand (which is not overall hours but rather “how hurried or rushed was the pace of the workday?”) would be higher now for many specialties, including mine. It’s a different world out there with the physician shortage and a strong corporate practice model.
I also wonder about the impact of Physical Demand on PTL here. For so many doctors, it’s precisely the lack of a physical component (i.e. being sedentary/anchored to a computer all day) that is a negative factor.
Jeff Goldsmith in “What Can We Learn from the Envision Bankruptcy?“:
Strategically, the Envision bankruptcy raises anew the question of whether there are economies of scale, and investment returns to scaling, in healthcare. Certainly the conventional wisdom argued that large firms like Envision had the ability to recruit and retain clinicians across vast geographies, and negotiating power with the large insurers that increasingly dominate key insurance sectors like Medicare Advantage and Managed Medicaid.
Envision’s demise strongly suggests that the power balance-both political and economic- has tipped decisively in the direction of payers like United. Rising interest rates, the increasing scarcity of clinicians as workaholic baby boom vintage docs and deepening financial challenges for the ultimate customers of many of these companies, namely hospitals, suggest that we may have reached an inflection point in the viability of many private equity physician care models, with their 4-7 year holding periods and a succession of owners. Current owners might find it increasingly difficult to exit their positions.
Here’s a passage from another op-ed about the reality that conventional preclinical medical education isn’t really working, titled: “Medical students aren’t showing up to class. What does that mean for future docs?”
We believe the immediate next step for preclerkship medical science medical education is clear. A flipped classroom, and thus an increased role for virtual learning in the preclerkship years of medical school, is a promising model. Can we preserve the broad goals of preclerkship medical education while supporting medical students in a decision they have already made to learn on their own time? We believe the answer is yes.
I constantly hear this refrain in education circles. The lecture is dead! Long live the flipped classroom! PBL! TBL! These are the cries of people who need the status quo to persist. People whose job is to how best fit the education of students into a box of X months without a big hit in USMLE passage. This story isn’t new. Versions of this op-ed have been cropping with increasing frequency for the past 10 years.
The concept of the “flipped classroom” is thus:
In this model, the in-person lecture all but disappears, and students learn most of the classroom-type material on their own before in-person time — hence the flip. We suggest starting with a series of virtual modules to prepare for case-based small group sessions held in person. Activities such as anatomy lab, patient interviewing and physical exam practice and special guest lectures would remain in-person. This, in essence, embraces the virtual lecture trajectory but requires actual attendance for small group hands-on learning.
Medical Schools are steadily moving in this direction. In Range, David Epstein discusses the futility of the current approach, the need to teach understanding/flexibility, and to not be so precious with our tools:
A team or organization that is both reliable and flexible, according to Weick, is like a jazz group. There are fundamentals—scales and chords—that every member must overlearn, but those are just tools for sensemaking in a dynamic environment. There are no tools that cannot be dropped, reimagined, or repurposed in order to navigate an unfamiliar challenge. Even the most sacred tools. Even the tools so taken for granted they become invisible. It is, of course, easier said than done. Especially when the tool is the very core of an organization’s culture.
Schools are willing to rethink a narrow tool like the lecture, but they are unwilling to step back and broadly reimagine what an effective and efficient medical education would really look like. Our conceptions of medical training are path dependent and therefore narrowly contrived. Would we do things this way if we didn’t have a century of entrenched history funneling us through the status quo? If you were designing from scratch, what would you do?
Burn it Down
In reality, the preclinical years should be standardized, competency-based, and largely offloaded to colleges. Being a premed should mean you’re actually working toward medicine and not playing status games pretending to care about vaguely relevant science. Medical school should be cheaper and shorter. I don’t care if it takes you three years or 3 months or nothing at all to be ready to pass Step 1. Medical school should basically start with a few months of Step 2 CK-type material and the clinical skills/reasoning components that are intermittently peppered into the first two years. Then clerkships.
The current paradigm was dumb in the age of Google. It’s asinine in the age of Chat-GPT.
We cannot possibly justify our current preoccupation with nearly useless microdetails.
We cannot simply combat the improvement in study techniques and third-party resources by making the tests more challenging. It’s an arms race that burns out students and distracts from training real doctors.
In a current four-year curriculum, there is so much waste: as much as two years inefficiently spent doing the basic sciences and a final year often mostly spent applying to residency and then attempting to relax as much as possible before the brutality of internship (yes, I’m aware that this is a sweeping and somewhat unfair generalization; it is nonetheless broadly true).
I am less interested in credentials—acquired by spending money and time—and more interested in results. We are past the point where using time as a proxy for competency is an appropriate argument. Doctors benefit from a wide moat protecting our profession, and those with keys to the kingdom obviously have an incentive to perpetuate the status quo.
But:
We are producing too few doctors for too much money during a process that takes too much time and is too unpleasant to result in a sufficient number that actually like their jobs, like their patients, and plan to have a long and productive career.
A Brittle Education
My point here is probably better made by Arturo Casadevall via Epstein (also in Range):
When Casadevall described his vision of broad education on a professional panel in 2016, a copanelist and editor of the New England Journal of Medicine (an extremely prestigious and retraction-prone journal) countered that it would be absurd to add more training time to the already jam-packed curricula for doctors and scientists. “I would say keep the same time, and deemphasize all the other didactic material,” Casadevall said. “Do we really need to go through courses with very specialized knowledge that often provides a huge amount of stuff that is very detailed, very specialized, very arcane, and will be totally forgotten in a couple of weeks? Especially now, when all the information is on your phone. You have people walking around with all the knowledge of humanity on their phone, but they have no idea how to integrate it. We don’t train people in thinking or reasoning.” Doctors and scientists frequently are not even trained in the basic underlying logic of their own tools. In 2013, a group of doctors and scientists gave physicians and medical students affiliated with Harvard and Boston University a type of problem that appears constantly in medicine: If a test to detect a disease whose prevalence is 1/1000 has a false positive rate of 5%, what is the chance that a person found to have a positive result actually has the disease, assuming you know nothing about the person’s symptoms or signs? Assuming the test detects every true case, the correct answer is that there is about a 2 percent chance (1.96 to be exact) that the patient actually has the disease. Only a quarter of the physicians and physicians-in-training got it right. The most common answer was 95 percent. It should be a very simple problem for professionals who rely on diagnostic tests for a living: in a sample of 10,000 people, 10 have the disease and get a true positive result; 5 percent, or 500, will get a false positive; out of 510 people who test positive, only 10, or 1.96 percent, are actually sick. The problem is not intuitive, but nor is it difficult. Every medical student and physician has the numerical ability to solve it. So, as James Flynn observed when he tested bright college students in basic reasoning, they must not be primed to use the broader reasoning tools of their trade, even though they are capable.
But tennis is still very much on the kind end of the spectrum compared to, say, a hospital emergency room, where doctors and nurses do not automatically find out what happens to a patient after their encounter. They have to find ways to learn beyond practice, and to assimilate lessons that might even contradict their direct experience.
Chris Argyris, who helped create the Yale School of Management, noted the danger of treating the wicked world as if it is kind. He studied high-powered consultants from top business schools for fifteen years, and saw that they did really well on business school problems that were well defined and quickly assessed. But they employed what Argyris called single-loop learning, the kind that favors the first familiar solution that comes to mind. Whenever those solutions went wrong, the consultant usually got defensive. Argyris found their “brittle personalities” particularly surprising given that “the essence of their job is to teach others how to do things differently.”
Science students learned the facts of their specific field without understanding how science should work in order to draw true conclusions.
“Brittle” is an amazing description of modern medical education.
The Ground Truth
Students have largely replicated and replaced the classic preclinical curriculum with outside tools. Those using the school’s resources are doing so for convenience, inertia, or the importance of the instructor’s idiosyncrasies for exams. The university model has been leapfrogged and has lost whatever stake it can plausibly claim with regard to teaching the basic sciences. There is so much that medical schools can and should do. But lecturing medical students about biochemistry is no longer one of them. We can’t justify a time-based curriculum and six-figure cost of attendance for the handful of students that enjoy going to class.
The flipped classroom is, in part, just fine: students do need in-person reinforcement of material, and there are real benefits of social connection with peers (and maybe even faculty!), but there is no way to turn the typical preclinical curriculum into a good use of time and money just by telling people to learn from Osmosis, Lecturio, Amboss, or Sketchy and hang out for an inefficient “work through the case” exercises with your peers because “healthcare is a team sport.”
The current gauntlet is so long, inefficient, and unpleasant that we are graduating doctors who have already lost their love of medicine and training residents who already have an eye on retirement. We are doing it wrong.
The Department of Justice said the defendants allegedly defrauded programs used to take care of elderly and disabled people, and in some cases used the ill-gotten money to buy exotic cars, jewelry and yachts.
DOJ busts $2.5 billion healthcare fraud scheme.
From “Research Fever—An Ever More Prominent Trend in the Residency Match”: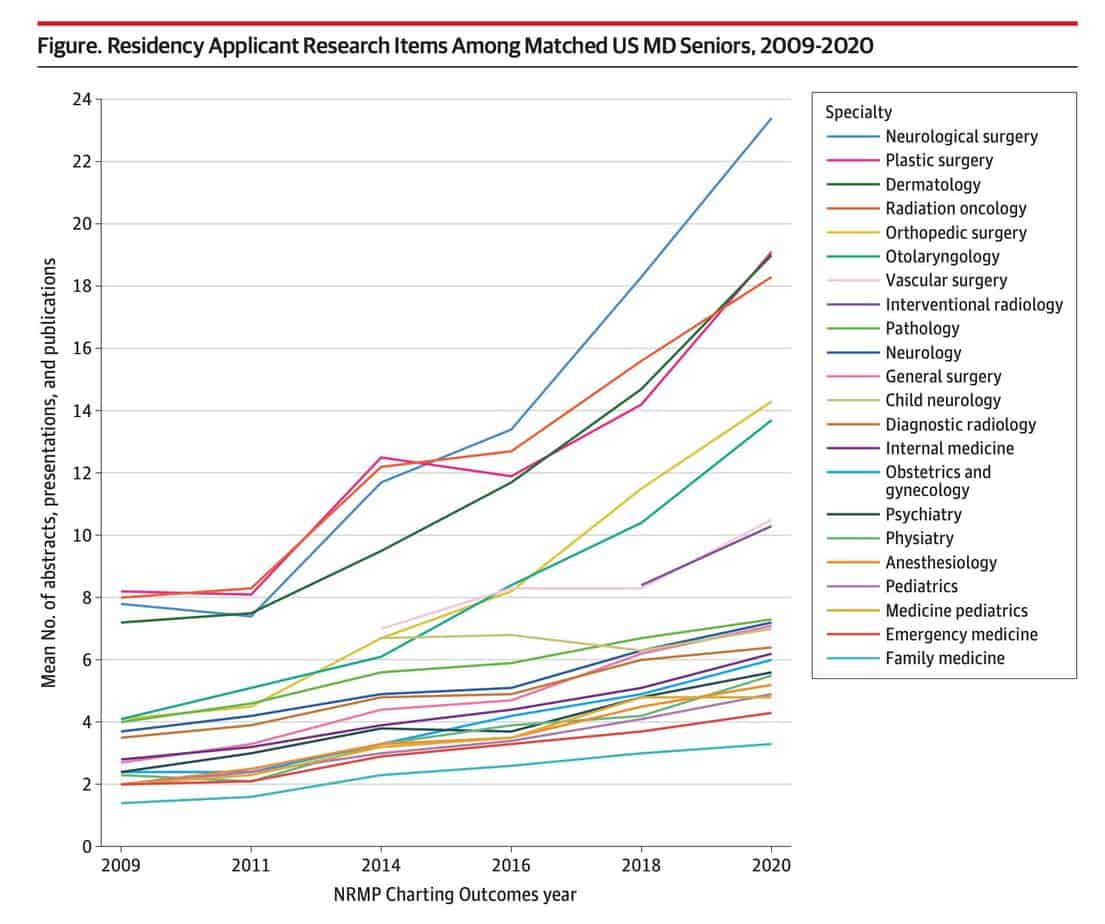
Insanity.
I have zero doubt that this incredible trend reflects a whole bunch of meaningless CV-fluffing that only further detracts from the mission of graduating good doctors.
I also wonder how much the bigger numbers in ERAS even impact individual success. Yes, studies have demonstrated that matched applicants on average have a greater number of research experiences than unmatched applicants, but how much can we attribute to the research and how much is just confounding correlation?
Other research has suggested that putting up big numbers during training doesn’t ultimately reflect those who go on to do research over the long term. It’s mostly brownie points and free trips.
At this point, we’d probably be better off with a residency lottery.
The pull of these forces left many doctors anguished and distraught, caught between the Hippocratic oath and “the realities of making a profit from people at their sickest and most vulnerable.”
Not only are clinicians feeling betrayed by their leadership,” she says, “but when they allow these barriers to get in the way, they are part of the betrayal. They’re the instruments of betrayal.”
From “The Moral Crisis of America’s Doctors.”
Speaking of physician shortages, Tennessee just became the first state to pass legislation allowing international medical graduates to obtain licensure and practice independently without completing a U.S. residency program. Bryan Carmody breaks it down.
It took a few years before it finally got there, but massive private equity-owned physician staffing company Envision finally filed for Chapter 11 bankruptcy this week.
The harbinger of the coming wave of PE defaults, bankruptcies, distressed exchanges, and other failures has fully arrived. Make no mistake, this is just the beginning.
There are people who see this news and rejoice. It’s not hard to see why. There might be more than a bit of schadenfreude seeing a big private equity company go belly up. These entities are so often in the business of pure value extraction. They aggressively use leverage to buy a bunch of stuff using a bunch of borrowed money and try to increase profits through negotiating clout, suppressed salaries, and unsavory financial machinations. They often take successful companies and saddle them with so much debt that they fail, strip them for parts, and let everything fall apart after they’ve made sure they made their buck. Many of the big retail failures of the past decades have all been the same story.
Envision was in the process of the usual playbook of financial machinations to separate the profitable wheat from the debt-riddled chaff when the WSJ reported on the possible impending bankruptcy and forced their hand.
Because such a large portion of their purchases are funded through debt, it’s relatively rare that the PE-owner actually loses a ton of their own money in the process. Envision’s owner KKR wasn’t quite so lucky: while the levered buyout was almost $10 billion in 2018, they are still likely to lose their entire ~$3.5 billion stake.
A Fall Long Coming
Envision’s reimbursement games didn’t pan out, not just their ploy of going out of network to charge exorbitant rates to unsuspecting patients—a practice curtailed by the No Surprises Act—but also from the bad acting of big payers like UnitedHealthcare (there are very few good guys in healthcare). Adding insult to injury, they weren’t able to squeeze physicians and other staff in the hot job market. Labor costs have been going up.
While Envision as a normal business is functioning, valuable, and generates cash, its growth was nowhere near the level required to service its more than $7 billion of debt. If the credit markets were loose like in the pre-Covid era, they probably would have been able to refinance without issue. Now, the cost of capital is simply too expensive.
This possibility was in the news back during the early Covid days, but Envision was temporarily saved by an influx of cash from the CARES Act. They recently defaulted on their debt and subsequently filed for Chapter 11 bankruptcy on May 15.
From the announcement email from Envision CEO Jim Rechtin:
Upon emergence from the restructuring, both Envision and AMSURG will be under new and separate ownership, comprised of current lenders. KKR will no longer have a stake in either company.
The email goes on to state the following items unironically:
- Envision and AMSURG are not going out of business. The filing ensures an orderly process for restructuring our debt and finances. This is not a liquidation.
- Our clinicians and clinical support teammates can expect to receive their normal wages and benefits. Independent contractors and locums can expect their usual payments.
- The filing does not change the regular work schedules of our clinicians or clinical support teams – operations will be business as usual.
- Our top priority is continuing to deliver high-quality care and supporting our hospital partners and surgery centers without interruption to services.
- There should be no change to the quality of service our patients and their families have come to expect from us.
As part of the process, Envision is now owned by its creditors (the lenders who had given secured loans and/or purchased corporate bonds,) and KKR has lost its stake and will no longer own/run the company. And it’s worth pointing out that nothing unsavory has really happened in the sense of business practice. This is how the industry is designed to work. People invest money and take on risk in order to make money. A company taking on debt it knows it can’t really afford and other unnecessary/excessive risks that might screw over its creditors is part of the game. When companies fail, the creditors get the scraps before the equity owners/shareholders.
Billions of dollars have been lost, absolutely, but at the end of the day, it’s mostly big institutional investors like large pension funds that are the ones who have lost in the short term. KKR made a bet and lost. They’ll be fine.
Of interest to most physicians is that the day-to-day function of Envision probably won’t change much, and this big company that got big by borrowing an unsustainable amount of money to fund its growth still exists. It may even emerge from this process potentially stronger than recent years now that it won’t have billions of dollars on the balance sheet and the need to make periodic debt payments. They will probably not be able to raise more capital in the current environment, which will prevent the kind of debt-fueled highly-leveraged growth that allowed a company like Envision to buy large practices in the first place. And their management record still does not inspire confidence. But at the end of the day, Envision as an entity is still big, still employs thousands of doctors, and still has a dominant market position in several locales. If there is any physician staffing company that could be considered too big to fail, Envision is one.
You might ask, why would Envision’s creditors take the deal? Is losing billions of dollars fun? Well, no. This is the nature of distressed exchanges: better to lose a few billion and end up with a big profitable company at the end than lose all of your billions.
What Next?
From the official FAQ:
How will patients be impacted?
Patients will continue to receive the same high-quality, high-value care our clinicians and physician partners have always provided. Patients and their families should notice no difference in our operations or level of care.
This is why those hoping that the collapse of private equity-funded healthcare ventures will lead to a return to better times are unfortunately in for a grim reality check. The tactics and market consolidation don’t have to go away just because they can’t pay their debts. We’re not likely to undo any damage already done. For better or worse, these companies will mostly soldier on. The playbook lives to see another day.
Unless physicians quit in droves on principle or in fear, the status quo continues. If people take the wake-up call about the flaws in the funding model, that’s a different story.