Another paper suggesting that clinicians prefer some structure (but not too much structure) in radiology reports. There are always edge cases where structured reporting becomes cumbersome–and overly parsed reports are also inefficient/unreadable–but there’s no denying it’s so much easier for me to scan a prior report when it’s not narrative free text.
A reader asked if anyone had successfully started a new radiology private practice recently, particularly one that involved financing, opening up new imaging centers, and fresh payor contracts. There is a vacuum in some areas, especially with the PE-exacerbated instability, and therefore a clear opportunity to those who can muster the manpower (no easy feat).
As a follow-up, I thought I’d ask (on their behalf): is anyone who has willing to mentor other upstarts?
The battle between Radiology Partners and UnitedHealthcare has ended with United as the victor.
The summary:
- RP claimed United owed them lots of money for underpayment because United was using a 2020 contract to determine some of its payments instead of a more lucrative 1998 contract originally held by one of its purchased groups, Singleton.
- United then sued Radiology Partners alleging an illegal pass-through billing scheme. It’s a good read.
- The arbitration panel awarded RP an interim award of $153 million. This was very much interim, not just because the independent panel had awkward bias conflicts, but also because the panel decided to separate the question of whether Singleton’s lucrative contract was in effect (it was) and if RP was abusing it (which it was) into separate steps.
The $153 million award would really have only been an extra $94 million since United had already paid for the work at a lower rate. (Author’s note: That’s quite the contract.)
Phase III—that awkward fraud question—just finished. The ultimate findings of the panel (free login required):
In the Phase I Decision entered on April 2, 2023, the Panel made the following finding: “The Panel finds the 1998 contract to be the operative agreement between the parties.” The Panel confirms this finding.
In Phase II the Panel entered the Interim Award On Singleton’s Arbitration Demand on September 26, 2023. The Panel now vacates that Interim Award.
The difference between the amount United paid on claims pursuant to the rates specified in the 2020 Agreement and the amount it would have paid pursuant to the rates specified in the 1998 Agreement is $94,275,324.00. United’s underpayment of Singleton’s claims at the rate specified in the 2020 Agreement was a breach of the 1998 Agreement.
Because of its breaches of the 1998 Agreement and its other acts and omissions, Singleton is not entitled to recover this difference and underpayment or any other relief against United. Because of its breaches of the 1998 Agreement and its other acts and omissions, United is not entitled to any other relief against Singleton. The Panel determines that the evidence fully supports these decisions at law and in equity.
Translation: you are both jerks, you are both wrong in your typical unique and despicable ways, please go away forever:
United was wrong to unilaterally use the incorrect contract to determine payments. RP was wrong to hide its ownership and then essentially pretend that every group in the region it owns was Singleton when they clearly weren’t.
(For more description/backstory, see the previous two posts: United against Radiology Partners & United is Still Fighting Radiology Partners.)
For those keeping score at home, United’s lawyer was correct when they said, “We do not agree that Singleton will recover an award from UnitedHealthcare.”
In other news, whether or not they were right, United is still a terrible company.
Or, “Why Independent Radiology is different from most job boards (but also still boring)”
So recently I created a simple, small website called Independent Radiology. It’s a boring job board, but it’s also different from most job boards.
Jason Fried from 37signals (makers of Basecamp, HEY, and other stuff) argued years ago that software should be opinionated. A random WordPress website isn’t software per se, but I feel as a random dude on the internet with a full-time job, family, writing avocation, etc that anything extra worth doing in this sphere is only worth doing if it’s going to help someone and is unabashedly done the way I would do it. It’s a project that reflects my biases, preferences, and mission. It’s idiosyncratic. It’s opinionated.
The Context
When I first thought seriously about the issues with the ACR job board earlier this year that inspired this project (now significantly improved, you’re welcome), I was partly irritated by disingenuous job listings from Radiology Partners that were masquerading as independent private practices. But I was also struck by several things:
Read More →
Something happened to the field of Radiology.
Actually, a lot of things have happened and are happening to Radiology all the time, but one of those things has been that the proliferation of corporate and private equity-backed radiology practices over the past decade has been followed by a historic radiologist shortage, a subsequent piping-hot radiology job market, and a challenging zero-sum game to hire on-site and even remote radiologists.
There are thousands of rad jobs available in the country and more work than the field can handle, but only a fraction of those positions are at independent radiologist-owned and controlled private practices. A lot are not.
That’s why I’ve temporarily been posting a radiology job ad on this otherwise very personal site, and that’s why I’ve just launched Independent Radiology.
From the “Why?” page:
The thriving independent private practice of radiology is critical to the future of the field. True private practice–where doctors control the organization, are responsible to their peers and patients, and earn the full fruits of their labor–is the benchmark that sets the market and provides the anchor against exploitation from unscrupulous employers.
This site exists to help those radiologists looking for the real deal.
You don’t have to agree with me, and you also don’t have to care. Not everyone needs or wants to work in private practice, and of course that’s fine. I also believe in the academic mission, and there’s nothing inherently wrong with being an employee. I also don’t want to just glamorize a practice model. Models aren’t destiny, and a private practice isn’t necessarily a good practice.
But, I do believe every radiologist should hope for the success of independent radiologist-owned private practices. The ability to join a thriving independent practice where doctors get paid for the full amount of their professional work and have the autonomy to choose how to do it is what forces employers to compete. It’s the anchor. It’s the BATNA that every hospital and corporate suit knows you have. It’s what keeps them honest.
By another analogy, the employment model is the renting to a partnership’s buying. There’s nothing wrong with renting. Renting can be great! Sometimes, based on your finances, the available options, and the local factors, renting is simply a better, safer option than buying. It’s undeniable. Not every house is a good purchase. And, when you have a good landlord, who charges you a fair market rate and is quick to fix the things that break down, renting can be an easy low-friction experience.
But we are stronger as a field when ownership is a real possibility. And, like homeownership, when you buy a good property, in the long run, you generally end up ahead. You have to deal with some upfront costs and the upkeep—oh, the upkeep!—but you also have more say about the property and you’re not reliant on someone else’s goodwill or business savvy. You have a good place to live: a home, not just a house. For the renter, the landlord can always change. They can always call your bluff and see how far they can push you before you decide to move. That’s why viable options are important for the whole market.
So, I wanted to make some space online to help those who want to join and help build a practice to find what they’re looking for. And, I wanted to build a place to showcase true independent radiologist-owned private practices in order to help them find radiologists in this challenging market.
I hope it’s helpful.
Should new residents worry about workflow efficiency and ergonomics?
Yes.
I don’t think it’s ever too early to start thinking deliberately about what makes you better and more efficient in your job or able to act more sustainably. If anything, spending more time on workflow and ergonomics early on in your career is an investment in yourself.
As a resident, I just used whatever was plugged into the workstation I sat at. This eventually led to wrist pain, which even more eventually led me to finally address my setup as an attending. The physical discomfort became obvious. The hit on my productivity/efficiency for all those years was invisible until I made the changes.
Many people, especially once out in practice, become entrenched in their behavior patterns and find it very difficult (and even frankly overwhelming) to approach changing how they work, even when the change is clearly beneficial.
I would say, on a practical level, that it may take some time after starting residency to know exactly what your needs are, what you like and don’t like about the default approach, and what an ideal workflow may be. But taking the basic step of buying a good mouse and programming it to help use PACS is an approachable and very helpful first step. At least do that, and then you can decide if you need to go down the rabbit hole.
The Approach
In general, you will find things easier especially as a resident if you can have a setup that requires no on-site software/driver installation, given the realities of bouncing around multiple workstations and the difficulties of working with your local IT department. Devices that can store their own settings and function plug-and-play on any computer are often described as having onboard memory.
I think a reasonable approach early on would at least involve some kind of gaming or productivity mouse to store window-level settings and your favorite PACS tools.
As you can see if you dive into my multi-post series, I personally divide these tasks between a left-hand device and a right-hand device and also incorporate dictation controls with Autohotkey. I think this is the optimal approach (and one that some of my residents have even now begun using). A dictaphone-free approach however really does require AutoHotkey to work efficiently, so utilizing this would depend on if you are able to get the executable file onto a workstation in order to run your shortcuts (or if the thing is locked down so tight that you won’t be able to). You may not know until you try or talk to someone local who has.
So, if you decide to take the streamlined approach and try to put all the PACS tools you want on a single device, you may find it helpful to have something with a large number of configurable buttons. A good example would be the reasonably priced UtechSmart VenusPro (a 16-button wireless mouse that includes a 12-button thumb grid). The G604 Lightspeed would be another popular choice (more expensive, adjustable scroll wheel, 6 thumb buttons). I personally use a “vertical” mouse, and I discuss even more mouse options (and everything else) at length in my “best stuff” post. (My hospital mouse is the very inexpensive Zelotes—which I describe how I use here—but it won’t be for everyone.)
Unless your radiology department is more forward-thinking and responsive than most, whatever is plugged into your computer is unlikely to be a good mouse for utilizing PACS. Even if it is, it probably isn’t configured the way you want, so literally any variety of productivity or gaming mouse that you customize yourself will provide some obvious and immediate benefits. The ultimate goal is that you should not need to move your hand off your mouse (or put down your microphone) in order to use a keyboard for routine actions.
If you need to touch the keyboard for every case, I would say you’re doing it wrong.
How Many Buttons Do I Really Need?
Good question. Everyone is different.
Some potentially very helpful shortcuts will vary a little by how your PACS handles measurements and things like zoom/pan. Some PACS automatically incorporate a manipulation tool like zooming into the central mouse wheel click or holding left/right mouse buttons simultaneously, whereas others require a keyboard shortcut. Some PACS will automatically helpfully change what the right click does depending on which PACS tool is active. Others do not. Some PACS delete measurements by double-clicking, and some make you press the delete key. That’s why it can be challenging to completely figure out what you want without some trial and error and becoming familiar with your local enterprise software function.
But here is one version:
Four window/level presets are probably sufficient for most people’s needs (e.g. soft tissue, lung, bone + brain or liver or your fourth favorite).
Some common choices for mouse button shortcuts are the measure tool, the ROI tool, delete, localizer/3D cursor to cross-register findings, and whatever button you need to turn back on power scrolling. Again, the exact details vary by PACS. That’s ~five more.
Most people would find the angle tool or spine labeling to be less important, but obviously in some cases those are in constant use, etc. Some PACS have a dedicated toggleable navigation pane to see priors and image series.
Add those together (~12) and it’s not hard to see how one can go crazy and fill up the thumb grid on one of these mice with all tools you need, even if you aren’t trying to add toggling dictation + previous/next template fields as well (3 more).
I will admit that it can be hard to retain all of these in muscle memory, which is one reason why I like using both hands. I suspect a lot of residents are already learning so much and doing so many new things that a smaller number of inputs may be more likely to fall in the sweet spot of being helpful without being overwhelming—but if you’re willing to put the time and energy in, you can get a ton of mileage from a high-button mouse.
Regardless, there is no world where you wouldn’t rather at least change your window/level settings from your mouse instead of dropping your mouse to hit the numpad on your keyboard instead.
Ultimately, the more things become easy for you to do, the more frustrating it is when some task requires you to break your flow.
Take Home
I’m not suggesting you should go full nerd mode and spend a bunch of money.
But, yes, you should at least get a programmable mouse for work.
- Yes, I’ve started the process of creating a small dedicated job board just for independent radiologist-owned private practices. With all the corporate noise out there, I’m hoping we can connect radiologists looking for the real deal with those groups who are doing it. Still a ways to go, but feel free to reach out to me at ben@benwhite.com if your group is interested, and I’ll get back to you when things are ready.
- Separately, yes, for the first time in this site’s 15-year history, I’ve decided to run a real ad. Not a banner ad (and no images), but starting on June 1st, there will be a single monthly post featuring a limited number of true radiology private practices. I’ve temporarily changed this policy because of the radiologist shortage combined with the current less-than-stellar recruitment/marketing environment. I hope folks find it unobtrusive and even helpful; I’ll reevaluate in a year.
It’s recruitment season, the radiology job market is hot, and there’s a lot of corporate noise. I’m thinking of maybe starting the world’s smallest radiology job board right here, open exclusively to a limited handful of 100% independent private practices.
If your group is interested in advertising on this site (and also therefore supporting my writing), email me at ben@benwhite.com.
Recruitment is a big challenge. While the ACR subsequently addressed the issue I wrote about here, I originally had the idea because of this.
When you first get into practice and really want to make a good early impression, you’re going to make some mistakes, and some of them are going to be pretty boneheaded. Everyone has holes in their knowledge, and there are almost certainly things that you should know that you somehow don’t.
Depending on your practice—and how often people see your name—it’s possible you may even burn a bridge or two with an experienced (or headstrong) clinician when you miss some key finding or raise alarm bills that didn’t need to be raised (especially when they end up causing them headaches in counseling their patients or dealing with the ER). You can’t change that first impression, all you can do is learn and improve and do better next time.
The frustrating reality is that an experienced clinician may have less general imaging experience than you do but plenty of targeted experience to answer most of their clinical questions as well if not better than you can when you first get out. Over time though, especially if you practice subspecialized or high-complexity care, you can eventually get to the next level.
With a good feedback loop including clinical follow-up to cement your knowledge, you’ll get more reps per day and spend more time reviewing each case than most clinicians seeing patients can hope to squeeze in. They will always have the patient in front of them and the clinical context that you will lack, so you will need to get better and better and better to become someone who they trust as much as—if not more than—themselves. I won’t pretend to know how many of the clinicians I work with respect me that much.
The End of Training is Just the Beginning
The practical reality is that residency/fellowship training are very important but also not always efficiently structured for practical learning. We tend to focus on the cases that hit the list every day—because there is work to get done—even though they may not be the ones that will teach us the most. We also tend to have research and procedures and other competing interests that distract from raw diagnostic radiology learning. And while reading cases out with an attending means that you get more reps of feedback than when working alone, both that and your limited experience means you will likely read fewer cases per day during training, even as a fellow, than you will as an attending.
For all of these reasons, the first six months (or two years, depending on who you ask) out of training can be a huge source of fear and anxiety but also a huge source of growth (especially if you are in a practice with high-quality colleagues that you can learn from and a healthy environment to get feedback in that will not crush your confidence).
Ultimately, the issue with learning after training is that there is no structure to make you put the extra work in, and you won’t necessarily receive feedback on most of the cases where you have the most to improve.
There’s No Forcing Function for Continuous Improvement
The sources for learning remain essentially the same: double down and read about the things that stress you out or slow you down during the workday, learn from the prior reports (especially when the person who read the case is better than you), and keep adapting your search pattern to incorporate your new knowledge and to address your mistakes.
Sometimes, adjusting your template or creating tailored macros can help you get more mental-checklist reps. For example, someone practicing neuroradiology could create a quick macro “pulsatile” that quickly runs downs the pertinent negatives for causes of pulsatile tinnitus that you invoke when that is the provided history, thereby forcing yourself to actively evaluate those causes on the images, thereby eventually making it an subconscious part of your process.
We could summarize this especially desirable kind of learning as deliberate practice. It’s simple to just get through the stack. Eventually, the muscle routines come no matter what, and you’ll gradually improve over your first five years in practice. But it’s harder to develop purposefully and improve in the specific areas you’re weak in if you don’t take a step back and figure out what are the primary causes of your errors and make sure your learning and working processes specifically address them.
So, The Phone Will Ring
For your entire career, every so often, you’ll receive a phone call asking you to take a “second look” at a case (or just flat out make an addendum). And that’s when you open it and see the obvious miss. Often that’s just human fallibility, but sometimes it will reflect a need to reevaluate your search pattern or recalibrate your chosen spot on the speed-sensitivity curve. That’s how we all (hopefully) get better over time.
Sometimes the finding is a tiny or questionable thing that is really only discernable with clinical context or history. Ideally, you’ll find every tiny Morton’s neuroma or extraforaminal disc protrusion, but sometimes it helps immeasurably to know what the actual history is and where to look. So be it.
And sometimes the doc will tell you what they think, and you’ll look at the images again, and you’ll still think you’re right. Hopefully, you’re humble enough to at least wonder if you could be wrong. That’s where having colleagues you respect can help a lot to be the tiebreaker. And sometimes, yes, the phone call is just a surgeon who wants to operate and needs you to provide an excuse. Even the bad actors can be right, so it still behooves you to treat every request with respect even when the clinician may not be.
This is something we all deal with, and the hardest part of that first year or two can be not taking it too hard. We interpret imaging for so many patients and touch a lot of lives, even though it sometimes doesn’t feel like it.
As much you can, try to remember: The ego matters less than the people behind the pictures.
In which we have the nonphysician CEO of the largest radiology company/practice in the country—one that employs 10% of the workforce, just received $720 million in rescue funding, and is valued at several billion dollars—taking the time to troll an individual radiologist on X (née Twitter):
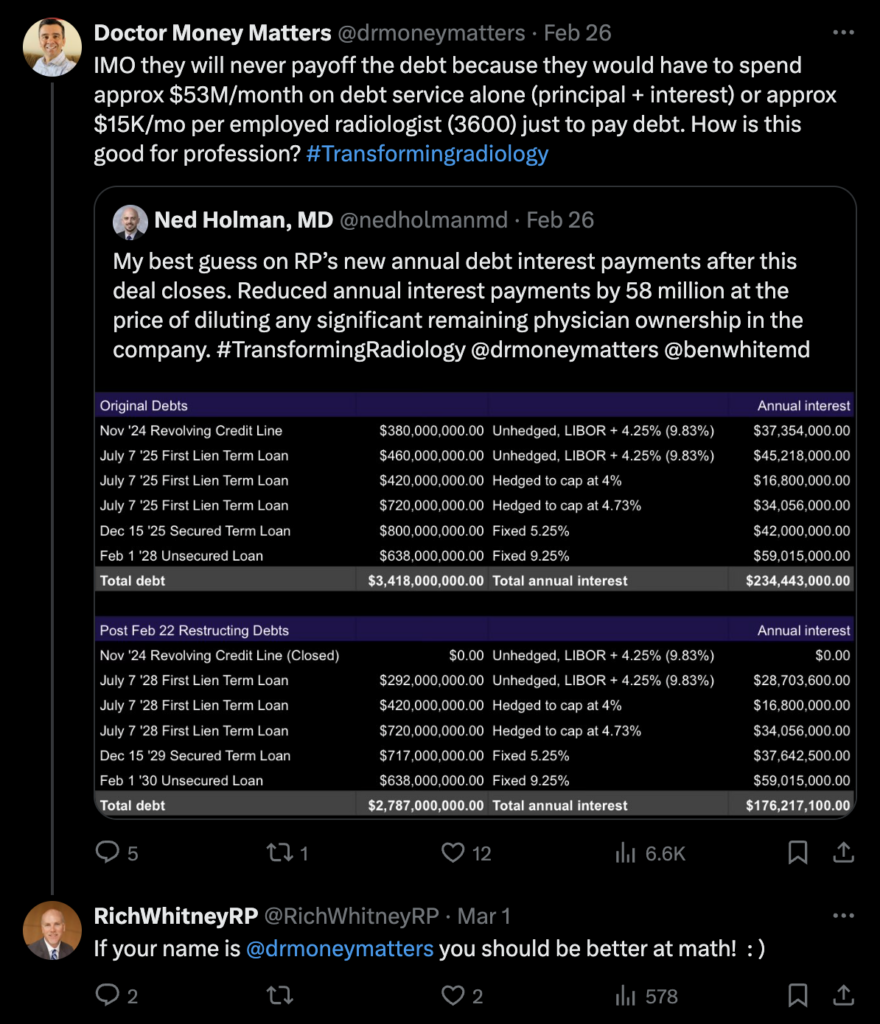
Clearly, a man delighting in his bailout.