If you’re an MS4, submit your ERAS today. Be the early bird.
And, when you’re done with that, you might prepare for the rest of the season with the Guide to Fourth Year.
If you’re an MS4, submit your ERAS today. Be the early bird.
And, when you’re done with that, you might prepare for the rest of the season with the Guide to Fourth Year.
This is another reader request and companion post to Studying for Third Year NBME Shelf Exams.
Let me start by saying that I’ve never personally utilized a detailed schedule as a binding contract. My ability to master my personal will with regularity is limited, and the day-to-day variability of a clinical workload makes strict planning difficult. You never know when you just don’t have it in you to work another moment.
That being said, there is some utility to making a rough outline in order to give yourself an idea as to how much time you have to complete various tasks, how many resources you can reasonably get through, and particularly, how much time to allot for dedicated question review at the end of the rotation prior to the shelf exam. You do not want to shortchange your time for questions. The details of your personal schedule will vary based on your clinical workload, the make-up/pain level of your clinical sites, and rotation length. Some schools do surgery in 8 weeks, others in 12. Length matters. Talk to students in the class above yours to get an idea of what kind of schedule to expect rotation to rotation.
The first step is to determine how many UW question sets you think you can do a single evening, assuming you’re working a normal schedule and are trying to achieve a measured pace and not kill yourself. I prefer to do tutor mode, and you may decide that you can reasonably achieve two full sections an evening with time for detailed review. Extrapolate based on your experience study for Step 1 to know what your speed and stamina can stomach.1
Let’s say you want to budget for 1 UW section (~44 questions) a night.
Let’s say you have a six week psychiatry clerkship.
This method will also allow you to determine what number of resources is reasonable/doable for you given your particular restraints. You can figure out if you have time to read a book twice or how to account for your desperate desire to read every book your classmates have mentioned. And while some days you may read more and others less, this method can help you keep on pace. Just make sure that if you start to get behind that you trim the fat: It’s more important to finish a single good resource than to pick away at parts of several, and you always need to give yourself time for questions.
Linkbait-y title aside, JAMA Internal Medicine has an interesting new too-small too-ungeneralizable study of 35 veterans across multiple VAs. In it, 49% (i.e. 17 patients) admitted that the availability of CT lung cancer screening reduced their motivation to quit. Reportedly, quitting is hard and CT scans are easy.
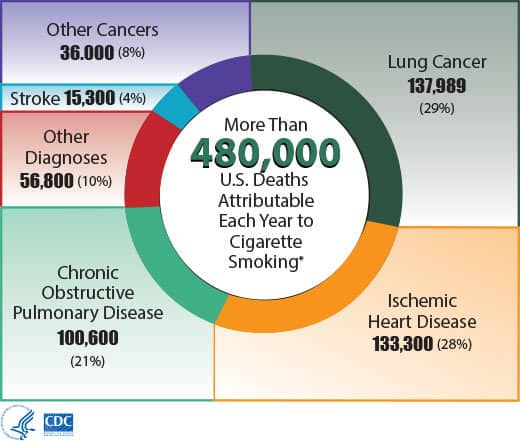
Of course, hunting for and even finding lung nodules isn’t going to prevent you from dying from cardiovascular disease or COPD, which together are responsible for over half of all smoking-related deaths. Nor will it touch the various other cancers smoking causes, like squamous cell carcinomas of the head and neck, which I see all the time. CT lung cancer screening for high risk individuals is a no-brainer, the data are substantial, but quitting or never-starting needs to be as well!
A couple of months back, JACR published an article with the self-evident conclusion that patients would prefer to hear the results of their radiology studies from their doctor (the ordering provider) instead of a radiologist. Duh! Who wants to hear they have cancer from a stranger who they may never see you again nor have any role in their future care?
Buried in that revelation is far more interesting and depressing data. While many patients don’t really understand the difference between ophthalmologists & optometrists and psychiatrists & psychologists, a substantial portion of patients essentially have no idea what a radiologist even is. The surveyed patients believed radiologists are techs who actually operate the machines and not physicians, and they comically underestimated the length of training:
While 88% of patients were confident they knew what a radiologist is and what one does, 79% thought they were technologists (misplaced confidence!). Only 56% knew radiologists are physicians, and even fewer, 31%, believed that radiologists perform image-guided procedures. On average, they believed that the speciality requires an average training of 6.8 years after high school. Respondents at community hospitals estimated even less time, 5.3 years, which would make radiologists second year medical students.
So even though I think it’s clear that patients would (and probably should) want to hear their results from the ordering physician, it’s even less surprising that they’d want the news that way if the alternative is to hear the results from a nonphysician who just finished their first year or medical school.
Here are the explanations for the updated 2015 (effectively 2015-16) official “USMLE Step 2 CK Sample Test Questions,” which can be found here.
Overall, there are a solid 41 new questions when compared with last year’s set, which I’ve marked with asterisks below. For those who have done last year’s set, a list of the new question numbers is in this footnote2. The explanations for last year’s set can still be found here.
If you’re looking for the answers to the newest June 2016 set, they’re available here. While the order is completely jumbled, there are only two new questions.
You should read my new free book on this subject.
Below are links to the original posts that make up my series on fourth year and the match:
For Step 2 CK/CS:
The more complete collection of medical school and residency related goodness (Step 3! Student loans! etc) can be found here.
Last updated April 2020.
Medical school is expensive and getting more so every year. Meanwhile, federal student loans are still at above market rates (and many private ones are predatory). Combine the two and a new doctor will borrow more and then pay more for the privilege than at any other time in history.
Over the past two years, historically low interest rates and a rebounding economy mean that private banks have re-entered the student loan business, particularly on the refinancing side.
As a resident, your options are essentially limited. Starting in March of 2015, DRB became the first company to offer a resident refinancing program that is unique, practical, and affordable for residents ($100 a month).
I wrote about refinancing as a resident at length in this post.
Otherwise, here is the complete picture for student loan refinancing.2
There are only a handful of options and the initial applications are short (really short, ~5 minutes or less). Rate ranges are typically concordant and are theoretically as low as the 2%-range variable across lenders. All quote you low rates assuming you’ll auto-debit from a checking/savings account. Initial applications will result in a soft pull on credit (does not affect your credit score) and give you a preliminary rate, so if you have good cash flow and can otherwise afford your loans (i.e. you’re an attending), you’ll do yourself no harm by simply applying for refinancing from each company and seeing which one is willing to refinance you at the best rate:
[This old page is here for archive purposes. I’ve removed the specific company references.]
Overall, the interest rate ranges offered by these companies are generally comparable. Typically when one lowers their rates, the others have followed quickly followed suit.2 The increasing competition in this space has been excellent for consumers, because the rates offered even a year ago weren’t that much lower than the federal ones. So, if you have several potential options based on your loan burden and your income, you might as well apply to all and see who gives you the best deal.3 Preliminary applications generally take 2-5 minutes, so there isn’t a big time investment in doing your due diligence. There are never any fees or costs to refinancing with any of these players, so you can refinance, keep an eye on the rates, and refinance again if they go down.
Bonuses: As mentioned above, I was able to convince several companies to provide a monetary incentive for you, dear reader, should you choose to refinance with them (in addition to a more standard referral bounty to me). I’m pretty pleased about that, as this allows you to effortlessly support me/this site as well as yourself.
From a UC Davis study that analyzed a >50,000 person national Medical Expenditure Panel Survey:
The study found that patients who were most satisfied had greater chances of being admitted to the hospital and had about 9 percent higher total health-care costs as well as 9 percent higher prescription drug expenditures. Most strikingly, death rates also were higher: For every 100 people who died over an average period of nearly four years in the least satisfied group, about 126 people died in the most satisfied group.
Interestingly, more satisfied patients had better average physical and mental health status at baseline than less satisfied patients. The association between high patient satisfaction and an increased risk of dying was also stronger among healthier patients.
Despite the proliferation of Press Ganey, I don’t think anyone who has worked in healthcare would find these results surprising. Healthcare may be a business, but there’s still trouble in treating patients like regular customers.
Dr. Daniela K Lamas, writing in the NYTimes:
My patient gave me a thumbs-up. I wished that I had known him better. “Cheers,” he said.

The future of prostate exam training is here, and his name is “Patrick.” Half sensor-embued tush-model and half computer-simulated cartoon-man, Patrick promises to grade medical students on their technique while also “present[ing] a realistic patient encounter” including “software that enables him to interact emotionally with the student.” (Before the exam begins, he tells you how scared he is.) [via Medical Daily]