Affluent conservatives often pat themselves on the back for having stable nuclear families. They preach that everybody else should build stable families too. But then they ignore one of the main reasons their own families are stable: They can afford to purchase the support that extended family used to provide—and that the people they preach at, further down the income scale, cannot.
[…]
For those who have the human capital to explore, fall down, and have their fall cushioned, that means great freedom and opportunity—and for those who lack those resources, it tends to mean great confusion, drift, and pain.
From conservative columnist David Brooks’ “The Nuclear Family Was a Mistake” in The Atlantic.
Even in medicine, we are seeing a disturbing trend. While the mean and median student debt are rapidly increasing due to high tuition rates, this is actually partially masked by the increasing percentage of medical students graduating with no debt. This suggests that a greater fraction of students come from means and have family support to cover medical school’s incredible cost. And those without that family support are either not getting in or are looking elsewhere.
It doesn’t stop at admission. These disparities and resource differences play out in specialty selection as well:
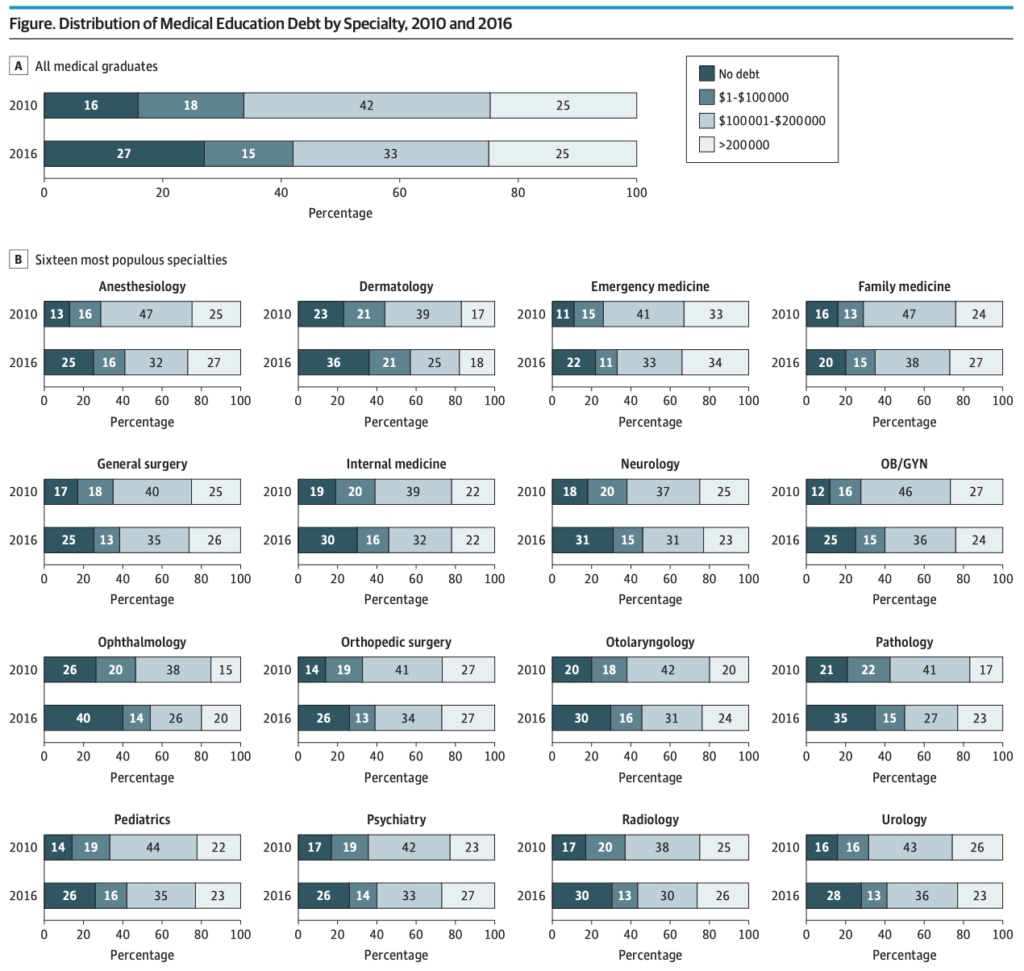
Over just a six-year period, the number of debt-free graduates almost doubled. And, overall, more competitive specialties like ophthalmology, ENT, urology, radiology have substantially more debt-free graduates than family medicine. Yet, we know we have a specialization problem in medicine. Free tuition at NYU isn’t going to change this massive headwind. The system needs retooling from far, far earlier.
4 Comments
On your chart by specialty, the main trend I see is that FM graduates have significantly more debt vs everyone else, not that the more exclusive subspecialties have less debt than everyone else. Eg, the fraction in IM w/o debt is 30%, the same as ortho, vs only 20% in FM.
Not disagreeing with your thesis, just saying. I always did have the notion that med studs who get into more lucrative specialties do so in part because they are better at signaling their status than other med studs. The easiest way to be better at this is to actually *have* higher SES from the get-go.
No, I agree. We say we want more FM, but we accept people who aren’t interested. The people who choose FM are more likely to be self-funded. Pricing out lower SES pushes the choices in the wrong directions by creating classes of doctors even more removed from the patients they treat.
As for IM, that’s confounded by the fact that it’s a stepping stone in many cases to other subspecialties.
I’ve always loved general adult medicine. I’ve always loved the hospital. I love hospitalists! I love rounding. I don’t even mind writing notes. I don’t even mind admitting new patients and writing discharge summaries, though it can get boring. But in private practice it looks much better than residency. But IM isn’t as lucrative as other specialties like surgical subspecialties. And people say you can’t be a hospitalist forever but I love it. If I were to subspecialize, I’d do critical care (no pulm), which is even more intense. What would burn me out is outpatient medicine! I say to each their own.